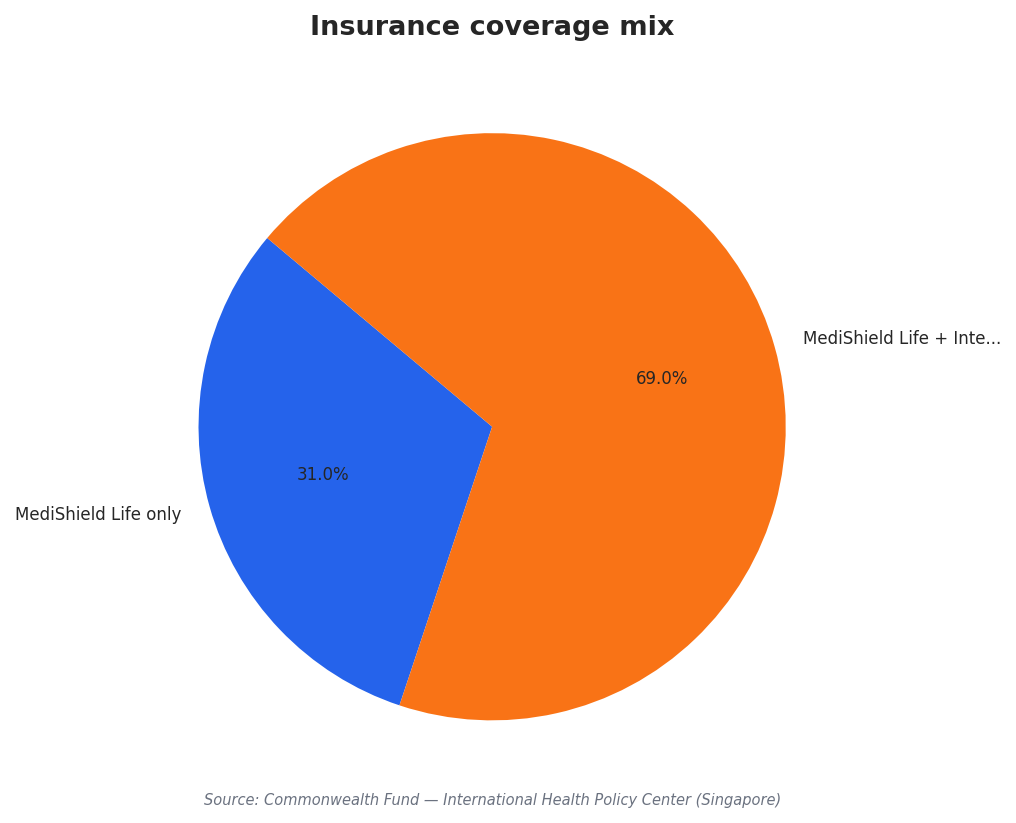
Singapore’s healthcare story is often told through beds, buildings, and waiting times. But rising demand also puts pressure on people: clinicians, coordinators, and support teams who keep care moving. The system already blends public and private participation, built on the “S+3Ms” financing framework: MediSave, MediShield Life, and MediFund. All Singapore citizens and permanent residents are covered by MediShield Life, while private Integrated Shield Plans are common supplements. The Commonwealth Fund reports that 31% of residents are covered by MediShield Life only, and 69% also hold Integrated Shield Plans. That coverage structure matters for the workforce because it shapes where patients seek care and how quickly care pathways can be navigated.
The demand picture is also changing because the population mix is shifting. TNGlobal reports that in Singapore, individuals aged 60 and above are projected to make up more than one-fifth of the population by 2030. At the same time, the Commonwealth Fund notes the nonresident population made up nearly a third of the population in 2024, and these individuals are not eligible for government subsidies and rely on employer-provided insurance that often falls short. The same source links this to a higher likelihood of seeking emergency care and more challenges with planned hospital visits and follow-up care, including leaving against medical advice and missing appointments. Those patterns can increase workload volatility and coordination effort, even when bed numbers do not change.
From Capacity Expansion to Workforce-First Operations
A workforce transformation is also an operations transformation. A ScienceDirect review describes Singapore’s National Healthcare Group C3 command center, deployed across multiple facilities during COVID-19 (2020–2022), saving over 2000 staff-days through automated inter-facility coordination and real-time capacity management. That is a workforce impact, not just a throughput metric. The same article points to examples where better process and coordination reduced strain without simply adding beds, and it references Singapore General Hospital’s technology-intensive bed management approach using RFID tracking, algorithmic allocation, and real-time dashboards to reduce bed-wait times at near-capacity utilization. The common thread is taking administrative load off staff and making decisions faster and more consistent.
Digital care models also reshape staffing needs and patient touchpoints. Hitachi Digital Services, citing an “Asia-Pacific Front Line of Healthcare Report 2022,” says Singapore anticipates a robust 26% surge in telehealth adoption from 2021 to 2024. In practice, higher telehealth use changes how teams are scheduled, how follow-ups are handled, and how escalation to in-person care is coordinated. Regionally, the same source highlights a looming shortage by 2030, with 4.7 million fewer healthcare workers in Southeast Asia and 1.4 million in the Western Pacific region (WHO Workforce 2030 Report). Singapore’s workforce planning therefore sits inside a wider labor market reality, where productivity, workflow redesign, and digital enablement become essential complements to recruitment.
Finally, infrastructure growth still matters, but it does not solve workforce bottlenecks on its own. Nexdigm describes a Singapore healthcare infrastructure market with growth drivers that include increasing healthcare demand, technology advancements, and investment in facility expansions and upgrades. Yet even in a system with strong public investment, staffing remains the binding constraint when demand rises. The Commonwealth Fund reports 165 primary care physicians per 100,000 inhabitants and 119 specialist physicians per 100,000 inhabitants, alongside government spending at 57% of health expenditure in 2022 and out-of-pocket spending at 25.4% of total healthcare spend. A practical Singapore healthcare workforce transformation in 2026 therefore looks like aligning financing, population needs, command-center coordination, and telehealth-enabled workflows so that scarce staff time is spent on care, not avoidable friction.
What is driving the need for Singapore’s healthcare workforce changes?
How did Singapore’s C3 command center affect staffing during COVID-19?
What does telehealth adoption mean for workforce planning in Singapore?
In the Singapore healthcare workforce transformation for 2026, what role do insurance and financing play?
What physician supply figures are reported for Singapore in the sources?